


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Remifentanil is a selective μ-opioid agonist with a rapid onset and very short duration of action. The μ-opioid activity, of remifentanil, is antagonised by narcotic antagonists, such as naloxone.
Assays of histamine in patients and healthy volunteers have shown no elevation in histamine levels after administration of remifentanil in bolus doses up to 30 μg/kg.
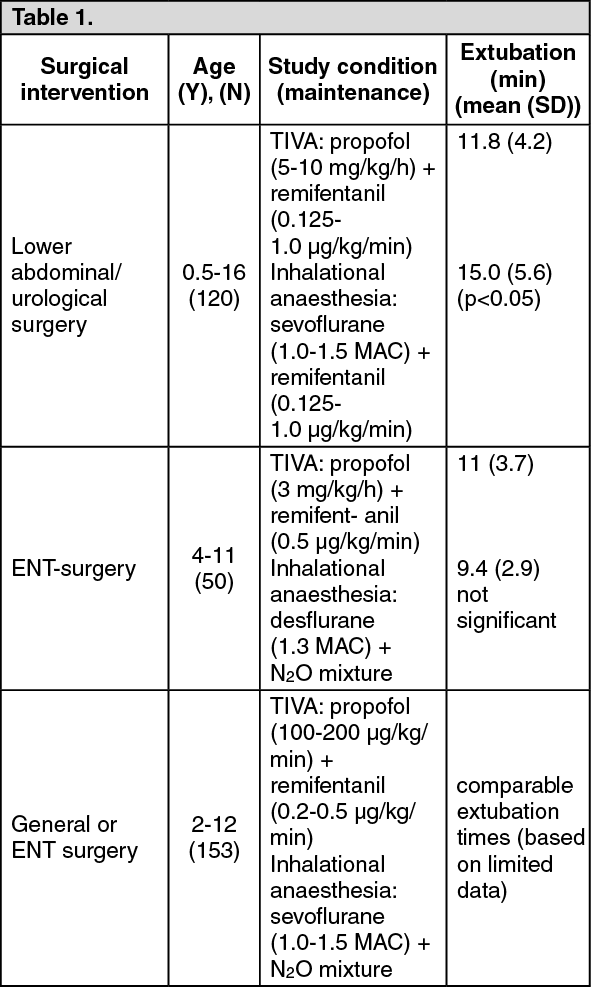
Neonates/infants (aged less than 1 year): In a randomised (ratio of 2:1, remifentanil:halothane), open label, parallel group, multicentre study in 60 young infants and neonates ≤8 weeks of age (mean 5.5 weeks) with an ASA physical status of I-II who were undergoing pyloromyotomy, the efficacy and safety of remifentanil (given as a 0.4 μg/kg/min initial continuous infusion plus supplemental doses or infusion rate changes as needed) was compared with halothane (given at 0.4% with supplemental increases as needed). Maintenance of anaesthesia was achieved by the additional administration of 70 % nitrous oxide (N20) plus 30% oxygen. Recovery times were superior in the remifentanil relative to the halothane groups (not significant). Use for Total Intravenous anaesthesia (TIVA) - children aged 6 months to 16 years TIVA with remifentanil in paediatric surgery was compared to inhalation anaesthesia in three randomised, open-label studies. The results are summarised in the table as follows. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the study in lower abdominal/urological surgery comparing remifentanil/propofol with remifentanil/sevoflurane, hypotension occurred significantly more often under remifentanil/sevoflurane, and bradycardia occurred significantly more often under remifentanil/propofol. In the study in ENT surgery comparing remifentanil/propofol with desflurane/nitrous oxide, a significantly higher heart rate was seen in subjects receiving desflurane/nitrous oxide compared with remifentanil/propofol and with baseline values.
Pharmacokinetics: Following administration of the recommended doses of remifentanil, the effective biological halflife is 3-10 minutes.
The average clearance of remifentanil in young healthy adults is 40 ml/min/kg, the central volume of distribution is 100 ml/kg and the steady-state volume of distribution is 350 ml/kg.
Blood concentrations of remifentanil are proportional to the dose administered throughout the recommended dose range. For every 0.1 μg/kg/min increase in i.v. infusion rate, the blood concentration of remifentanil will rise to 2.5 ng/ml.
Remifentanil is approximately 70 % bound to plasma proteins.
Metabolism: Remifentanil is an esterase metabolised opioid that is susceptible to metabolism by non-specific blood and tissue esterases. The metabolism of remifentanil results in the formation of an essentially inactive carboxylic acid metabolite (1/4600th as potent as remifentanil).
Studies in man indicate that all pharmacological activity is associated with the parent compound. The activity of this metabolite is therefore not of any clinical consequence.
The half life of the metabolite in healthy adults is 2 hours. Approximately 95 % of remifentanil as the carboxylic acid metabolite is recovered in the urine in patients with normal renal function. Remifentanil is not a substrate for plasma cholinesterase.
Placental and milk transfer: In a human clinical trial, the average maternal remifentanil concentrations were approximately twice those seen in the foetus. In some cases, however, foetal concentrations were similar to those in the mother. The umbilical arteriovenous ratio of remifentanil concentrations was approximately 30 % suggesting metabolism of remifentanil in the neonate. Remifentanil related material is transferred to the milk of lactating rats.
Cardiac anaesthesia: The clearance of remifentanil is reduced by approximately 20 % during hypothermic (28°C) cardiopulmonary bypass. A decrease in body temperature lowers elimination clearance by 3 % per degree centigrade.
Renal impairment: The rapid recovery from remifentanil-based sedation and analgesia is unaffected by renal status. The pharmacokinetics of remifentanil are not significantly changed in patients with varying degrees of renal impairment even after administration for up to 3 days in the intensive care setting. The clearance of the carboxylic acid metabolite is reduced in patients with renal impairment. In intensive care patients with moderate/severe renal impairment, the concentration of the carboxylic acid metabolite is expected to reach approximately 100-fold the level of remifentanil at steady-state. Clinical data demonstrate that the accumulation of the metabolite does not result in clinically relevant μ-opioid effects even after administration of remifentanil infusions for up to 3 days in these patients.
Up to now, data on safety and pharmacokinetic activity of metabolites after infusion of remifentanil for more than 3 days are lacking.
There is no evidence that remifentanil is extracted during renal replacement therapy.
The carboxylic acid metabolite is extracted during haemodialysis by 25 - 35 %. In patients with anuria the half-life of the carboxylic acid metabolite is increased to 30 hours.
Hepatic impairment: The pharmacokinetics of remifentanil are not changed in patients with severe hepatic impairment awaiting liver transplant, or during the anhepatic phase of liver transplant surgery. Patients with severe hepatic impairment may be slightly more sensitive to the respiratory depressant effects of remifentanil. These patients should be closely monitored and the dose of remifentanil should be titrated to the individual patient need.
Paediatric patients: The average clearance and steady state volume of distribution of remifentanil are increased in younger children and decline to young healthy adult values by age 17. The elimination half-life of remifentanil in neonates is not significantly different from that of young healthy adults. Changes in analgesic effect after changes in infusion rate of remifentanil should be rapid and similar to those seen in young healthy adults. The pharmacokinetics of the carboxylic acid metabolite in paediatric patients between 2 and 17 years of age are similar to those seen in adults after correcting for differences in body weight.
Elderly: The clearance of remifentanil is slightly reduced (approximately 25 %) in elderly patients (over 65 years of age) compared to that in young patients. The pharmacodynamic activity of remifentanil increases with increasing age. Elderly patients have a remifentanil EC50 for formation of delta waves on the electroencephalogram that is 50 % lower than young patients; therefore, the initial dose of remifentanil should be reduced by 50 % in elderly patients and then carefully titrated to meet the individual patient need.
Toxicology: Preclinical safety data: Remifentanil, like some other fentanyl analogues, produced increases in action potential duration (APD) in dog isolated Purkinje fibres. There were no effects at a concentration of 0.1 micromolar (38ng/ml). Effects were seen at a concentration of 1 micromolar (377ng/ml), and were statistically significant at a concentration of 10 micromolar (3770ng/mL). These concentrations are 12-fold and 119-fold respectively the highest likely free concentrations (or 3-fold and 36- fold respectively, the highest likely whole blood concentrations) following the maximum recommended therapeutic dose.
Acute toxicity: Expected signs of μ-opioid intoxication were observed in non-ventilated mice, rats, and dogs after large single bolus intravenous doses of remifentanil. In these studies, the most sensitive species, the male rat, survived following administration of 5 mg/kg.
Intracranial bleedings in dogs caused by hypoxia declined within 14 days after stopping remifentanil application.
Chronic toxicity: Bolus doses of remifentanil administered to non-ventilated rats and dogs resulted in respiratory depression in all dose groups, and in reversible intracranial bleedings in dogs. Subsequent investigations showed that the microhaemorrhages resulted from hypoxia and were not specific to remifentanil. Brain microhaemorrhages were not observed in infusion studies in non-ventilated rats and dogs because these studies were conducted at doses that did not cause severe respiratory depression. It is to be derived from preclinical studies that respiratory depression and associated sequelae are the most likely cause of potentially serious adverse events in humans.
Intrathecal administration to dogs of the glycine formulation alone (i.e. without remifentanil) evoked agitation, pain and hind limb dysfunction and incoordination. These effects are believed to be secondary to the glycine excipient. Because of the better buffering properties of blood, the more rapid dilution, and the low glycine concentration of the Remifentanil formulation, this finding has no clinical relevance for intravenous administration of Remifentanil.
Reproductive toxicity studies: Placental transfer studies in rats and rabbits showed that pups are exposed to remifentanil and/or its metabolites during growth and development. Remifentanil-related material is transferred to the milk of lactating rats.
Remifentanil has been shown to reduce fertility in male rats when administered daily by intravenous injection for at least 70 days at a dose of 0.5 mg/kg, or approximately 250 times the maximum recommended human bolus dose of 2 microgram/kg. The fertility of female rats was not affected at doses up to 1 mg/kg when administered for at least 15 days prior to mating. No teratogenic effects have been observed with remifentanil at doses up to 5 mg/kg in rats and 0.8 mg/kg in rabbits. Administration of remifentanil to rats throughout late gestation and lactation at doses up to 5 mg/kg IV had no significant effect on the survival, development, or reproductive performance of the F1 generation.
Genotoxicity: Remifentanil did not yield positive findings in a series of in vitro and in vivo genotoxicity tests, except in the in vitro mouse lymphoma tk assay, which gave a positive result with metabolic activation. Since the mouse lymphoma results could not be confirmed in further in vitro and in vivo tests, treatment with remifentanil is not considered to pose a genotoxic hazard to patients.
Carcinogenicity: Long term animal carcinogenicity studies have not been performed with remifentanil.